

As prophetically emphasized by one of my Dinka informants in 1986, 'to starve' is transitive: it is something people do to each other. (Alex de Waal, Famine that Kills, 2005 ed. p.xii)
This is the second in a series on trying to understand how to model the famine currently taking place in Sudan, in hopes of bringing more attention to the topic. Continuing from my previous post, where I looked at how to estimate the total number of calories available in Sudan, today I provide an overview of how to calculate caloric deficits, how these affect changes in weight, and how this leads to excess mortality (feel free to skip this one if you’re interested more in politics or conclusions, but it seems important to lay out the basics). In the final part of this series, I will put this together with a model of how calories are distributed among the population and, when insufficient, leading to hunger and malnourishment.
But before getting into the technical calculations, it’s worth keeping in mind the grim reality that we’re attempting to describe. I encourage readers to try to put a human face to the suffering of famine, and to try to imagine what it must be like to be a parent who cannot provide enough food for their children. Each of these stories is heartbreaking.
Many video reports are available, for example on youtube from the BBC or this report from PBS News Hour that includes an interview with a doctor in a hospital who treats children suffering from malnourishment (also available at the bottom of the page).
Population, BMI, and distribution of food
We will again be working to reproduce the approach from the Clingendael report1 that predicts millions of deaths from famines in the coming years in Sudan. The basic dynamic of the model centers around the relationship of the (in)availability of food and the resultant effect on the health of citizens, modeled as body-mass index (BMI in kg/m²), and the impact of low BMI on excess mortality. Each step in the process is complicated, but we will start with some simplifying assumptions and try to focus on the key relationships.
Here’s a quick overview of the full approach. In each month, we consider that an individual consumes a given amount of calories as a function of the overall food available and an assumed unequal distribution of the calories over the population (modeling each percentile of the population). As previously, we will focus on calories from grain and assume these make up 70% of all calories.2 When those calories are inadequate, the individual loses weight (BMI), and very low BMI levels lead to higher probability of excess mortality, according to a fixed formula (see below). Finally, we will model dynamically each percentile of the population for each month, keeping track of the effect on BMI, food stocks, and the population in each percentile, as a result of immigration, emigration, births, and deaths, including ‘excess’ deaths.
For today we will just focus on the caloric deficit, BMI and excess death calculations.
Notes
We will assume BMI is homogenous within groups, that is, no distinction by gender or age (but in fact there is good reason to think children have different caloric requirements3 and that women are better able to use all reserves then men4 )
The model of how BMI responds to caloric intake is based on studies focused on North America, and in conditions that may be unlike those of individuals in Sudan5
Physical activity changes caloric intake requirements.6
As previously, if you prefer to see the content in code, see the jupyter notebook here.
BMI change as a result of caloric intake
How one’s body responds to caloric restriction depends on one’s body mass index. Here we model month-to-month change, based on caloric deficit and the previous months BMI, following the methodology in the Clingendael report. First, caloric requirements depend on BMI as follows:
BMI<15: caloric requirements are 1900
15 < BMI < 18.5: caloric requirements are 2100 (the standard figure used in determining food aid requirements)
BMI > 18.5: caloric requirements are 2200.
Based on this, we calculate caloric deficiency as a percent of these caloric requirements. Finally we use this to calculate the amount that BMI changes over one month as follows:
To break this down, the first part says that the greater the caloric deficit, the greater the loss in BMI. However, the body responds in various ways to caloric deficits and weight loss by trying to conserve energy (homeostatic processes), so the second part of the equation suggests that this effect is somewhat mitigated by lower BMI levels.

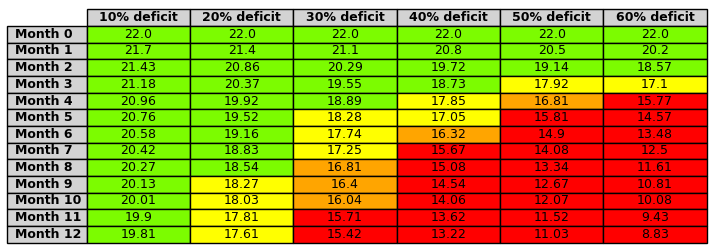
We can get a rough sense of the impact of famine by looking at how BMI changes over time, based on a fixed month-by-month caloric deficit over a period of 13 months.
Excess mortality as a function of BMI
The Clingendael reports using the following equation to fit to empirical results from previous research7:
One reference point is that as BMI gets below 16 (the WHO cutoff for the most severe category of “severe thinness”, the excess mortality in a given month approaches 1%. Naturally, there are many caveats to this - malnutrition can also lead to susceptibility to (infectious) diseases which can increase mortality rates within a community, etc.

Documentary - Inside Sudan’s civil war
The technical details above are a bit dry and abstract, and while they help us look at the big picture, we shouldn't forget that every individual’s loss is infinite.
Gaasbeek, Timmo. “Sudan: From hunger to death” May 24, 2024. Clingendael Alert. Clingendael Insitute.
So in months where less grain is available, each individual is assumed to consume correspondingly fewer non-grain calories as well. We might object that in months with less grain individuals would do more to procure non-grain calories, but that presumes a freedom of movement and action that is not presumably realistic. Future analysis might identify whether alternative treatment of this residual (non-modeled) variation is important.
Henry, C. J. K. 2001. “The Biology of Human Starvation: Some New Insights”. Nutrition Bulletin 26:3.
See the details of the studies in Henry, op cit.
Gaasbeek, op cit. For more details, see the 2001 FAO report on “Human Energy Requirements”, in particular Section 5.3 on activity level, which suggests that average people in less developed countries have requirements roughly 40-60% greater than those of us in developed countries, while strenuous activity can increase caloric needs by a factor of 2 or even 2.4 times.
Henry, op. cit, and Aune, Dagfinn, et al. "BMI and all cause mortality: systematic review and non-linear dose-response meta-analysis of 230 cohort studies with 3.74 million deaths among 30.3 million participants." BMJ 353 (2016).